

Understanding Medical Direction, Supervision, and the QZ Modifier
The questions every anesthesia practice should be asking are simple: Is your anesthesia billing compliant? Are you capturing every reimbursable opportunity? The answers, however, require a working knowledge of a modifier system that was designed for a healthcare landscape that no longer exists, and the financial stakes of getting anesthesia billing compliance wrong can be significant. Understanding how billing rules, medical direction, and the QZ modifier function in today’s environment is essential for protecting both anesthesia reimbursement and compliance.
The Origins of Modern Anesthesia Billing Rules
To understand today’s anesthesia billing requirements, it helps to understand why the rules were created.
In the 1990s, CMS faced a significant balancing act, needing to simultaneously address:
- Physician oversight
- CRNA utilization
- Rural access
- Cost containment
- Fraud prevention
The result was the anesthesia modifier system, a framework built around the concept of the Anesthesia Care Team, in which a physician anesthesiologist supervises or directs one or more CRNAs.
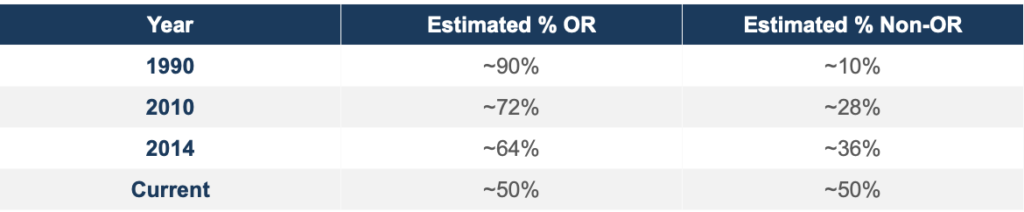
At the time, the framework made intuitive sense. In 1990, an estimated 90% of anesthesia cases were performed in the operating room. The environment was controlled, the care team structure was straightforward, and the rules mapped reasonably well to real-world practice.
The Growth of NORA Anesthesia and New Compliance Challenges
Today’s anesthesia services environment looks nothing like the 1990s.
Non-Operating Room Anesthesia (NORA), including care delivered in endoscopy suites, interventional radiology labs, electrophysiology labs, cardiac catheterization labs, and MRI suites, has grown dramatically.
Several forces have driven this transformation:
- Widespread adoption of propofol
- Advances in minimally invasive techniques
- Growth of interventional cardiology and radiology
- Explosion of GI procedural volume
- Broader shift toward outpatient medicine
Each of these trends has pulled anesthesia care out of the traditional OR and into environments that were never the primary focus when current anesthesia reimbursement and billing rules were written.
This historical mismatch is the root cause of many modern anesthesia compliance disputes, including disagreements surrounding QZ billing, concurrency limits, the scope of medical direction, and documentation requirements.
The Seven Steps of Medical Direction: All or Nothing
Under CMS rules, there is a meaningful difference between medical direction and medical supervision, and that distinction carries major reimbursement implications.
To bill under the medical direction model, a physician anesthesiologist must personally perform and document all seven of the following steps for each case:
- Perform a pre-anesthetic examination and evaluation
- Prescribe the anesthesia plan
- Personally participate in the most demanding procedures in the anesthesia plan, including induction and emergence (where applicable)
- Ensure that any procedures not performed personally are carried out by a qualified individual
- Monitor the course of anesthesia administration at frequent intervals
- Remain physically present and available for immediate diagnosis and treatment of emergencies
- Provide indicated post-anesthesia care
Failure to satisfy and document every required step can create significant anesthesia billing compliance risk.
Medical direction applies when an anesthesiologist is directing one to four concurrent anesthesia cases. Once that number exceeds four, CMS generally reclassifies the arrangement as medical supervision, a distinction that carries dramatically lower reimbursement.
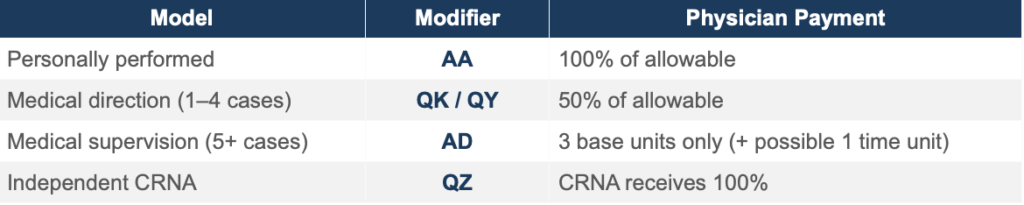
The financial contrast is significant. Consider a standard case worth 15 anesthesia units (7 base + 8 time). Under the personally performed model, the physician collects the full value of those 15 units. Under medical supervision, where the physician may be directing five or more simultaneous cases, that same physician might collect only 3 to 4 units total, while the CRNA bills separately using modifier QX.
Understanding concurrency thresholds is critical to both anesthesia reimbursement and revenue cycle management performance.
Understanding the QZ Modifier
Modifier QZ carries a specific and important definition under CMS:

This model is distinct from the team-based structures described above. It reflects an entirely separate care delivery model, not simply a documentation deficiency.
Recently, reimbursement for the QZ model has come under increased scrutiny from commercial payers, with many implementing a default 15% reimbursement penalty.
Common Anesthesia Billing Compliance Risks
The rules governing anesthesia billing were written for a world dominated by OR cases and traditional Anesthesia Care Teams.
The rapid growth of NORA anesthesia, combined with increased concurrency demands in busy practices, has created new compliance risks that many groups are not fully prepared to manage, or may force them to bill all cases under the QZ modifier and accept a 15% reimbursement penalty.
Common risk areas include:
- Practices that fail to document all seven steps of medical direction may inadvertently bill at a higher rate than their documentation supports.
- Practices that allow concurrency to drift above four cases without recognizing the implications may be misclassifying medical supervision as medical direction.
- Practices operating in non-traditional NORA anesthesia settings may lack the workflow infrastructure necessary to capture required anesthesia documentation.
The answer to the question, “Is your billing compliant?” starts with an honest assessment of documentation processes, scheduling patterns, and an organization’s understanding of where cases truly fall within the CMS framework, not where they assume they fall.
The Future of Anesthesia Billing Compliance
As the anesthesia landscape continues to evolve, maintaining strong anesthesia billing compliance practices is essential for protecting reimbursement and minimizing financial risk. Organizations that understand CMS anesthesia billing rules, monitor concurrency, and maintain accurate documentation will be better positioned to navigate ongoing changes in care delivery and payer expectations. With continued growth in NORA anesthesia and increasing scrutiny around modifiers such as QZ, proactive compliance oversight is no longer optional—it is a critical component of long-term operational and financial success.
References & CMS Authority
Primary CMS Sources:
- Medicare Claims Processing Manual, Chapter 12, §50
- 42 CFR §414.46
For additional guidance, see the Centers for Medicare & Medicaid Services (CMS) and the American Society of Anesthesiologists (ASA).
This article is intended for educational and informational purposes only. For billing and compliance guidance specific to your practice, consult a qualified healthcare attorney or certified anesthesia billing specialist.
Author:
Dr. Peter Goldzweig, DO FASA
Senior Physician Executive